Reliable service
Bariatric endoscopy
The different bariatric techniques manage to reduce the volume of the gastric cavity by means of endoscopic sutures or temporary physical means such as intragastric balloons.
For the treatment of overweight, obesity and weight gain we have the following services:
01.
Intragastric balloons
The intragastric balloon (IGB) is one of the most popular and effective endoscopic weight loss procedures available today. The material from which it is made is silicone.
The placement is minimally invasive, ambulatory and painless. Its implantation is generally performed assisted by a gastroscopy. It is introduced orally completely collapsed. When the balloon is found to be in the stomach, it is commonly filled with 500-600ml of methylene blue colored water.
The purpose of the gastric balloon is to occupy a significant volume in the gastric cavity, increasing early satiety and decreasing the feeling of hunger. As a consequence, there is considerable weight loss in a very short time.
There are multiple types of gastric balloons, their difference lies in the time they will remain in the gastric cavity. The duration of the balloon is scheduled for 6 or 12 months.
Judging by the associated complications, in my experience, no brand is superior to another in quality. Neither in weight loss. It has been shown that on average for 6 and 12 month old balloons, the percentage of total weight lost (%TBWL) is 15-18% (33 and 60 lbs)
– Overweight with a BMI between 27-30 kg/m² and comorbidities such as metabolic syndrome, arterial hypertension, diabetes
– Type I and II obesity (BMI 30-40 kg/m²)
– BMI > 40 kg/m² when:
– The patient refuses surgery
– There is a contraindication for surgery
– In the period prior to surgery to reduce surgical morbidity (especially BMI > 50 kg/m²)
– Patient who has undergone multiple diets and has not been able to lose >5% of total weight.
– Non-alcoholic hepatic steatosis (fatty liver)
– Pregnancy.
– Previous gastric surgery.
– Coagulopathies that require continuous use of anticoagulants.
– Hiatal hernia >5cm.
– Esophageal diseases: gastric varices, severe esophagitis.
– Crohn’s disease in the stomach.
– Drug addiction: Drug addiction and alcoholism.
– Uncontrolled psychiatric disorders.


02.
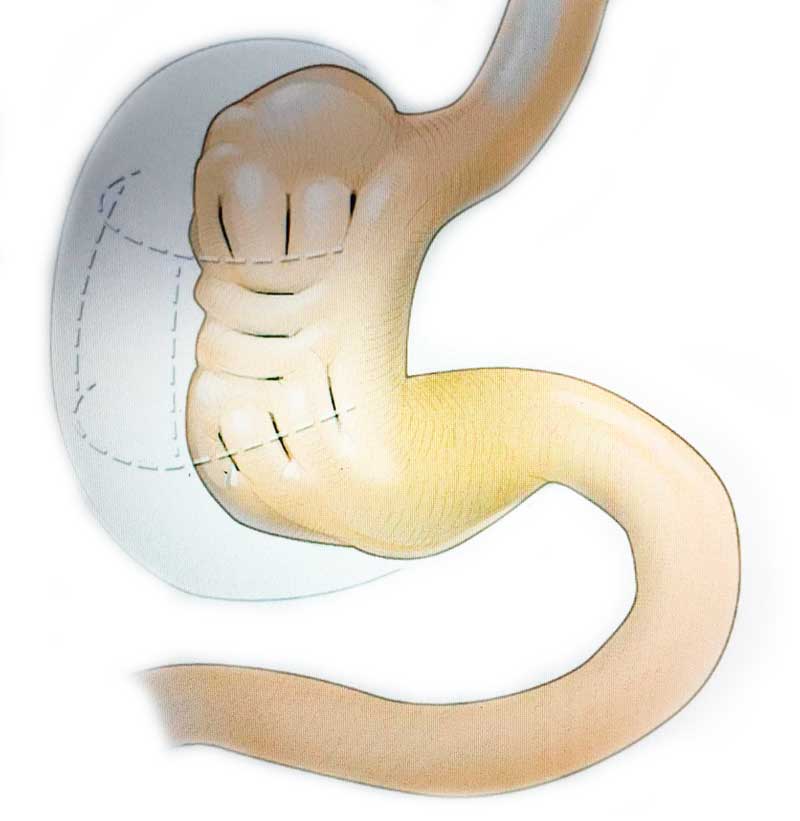
Endoscopic sleeve
The term endoscopic sleeve, also known as endoscopic gastroplasty, are alternative and minimally invasive techniques to traditional surgical options to reduce the size of the stomach. Specifically the endo-sleeve and endoSleeve method.
The endoscopic sleeve or GESP (Gastric sleeve endoscopic plication) is an evolution of the POSE® technique that consists of making up to 18 sutures in the stomach with a new pattern of plications similar to the surgical technique of the Sleeve or gastric sleeve.
The techniques are performed through the mouth to reach the stomach, achieving reductions of more than 35% of the gastric cavity, without external scars, it has good results and with minimal discomfort for the patient.
The stomach acquires the shape of a gastric sleeve through the formation of permanent and irreversible folds thanks to plications.
The procedure is indicated in people with type I and II obesity, that is, a body mass index (BMI) of 30 to 40 kg/m². The intervention takes about 35 minutes, recovery is fast and involves a hospital admission of 12-24 hours to better control the initial symptoms of pain and discomfort.
Generally speaking, they can have losses of between 33 and 77 pounds (15-35 kg).
For questions and budget
03.
Endoscopic treatment in weight gain
Over time, up to 30% of patients undergoing gastric bypass or gastric sleeve have regained practically all the weight they had lost. Surgical reoperation in these patients is more complex and has a high complication rate, which is why many patients reject it.
For questions and budget
Re-GESP
El GESP (Gastric sleeve endoscopic plication) es una evolución de la técnica POSE® (Primary Obesity Surgery Endoluminal).
La técnica Re-GESP consiste en reintervenir endoscópicamente aplicando el nuevo patrón de suturas a los pacientes que inicialmente fueron sometidos a una cirugía laparoscópica de Sleeve gástrico con consecuente dilatación de la cámara gástrica y reganancia de peso. El procedimientos tienen como objetivo reducir el volumen gástrico para conseguir una pérdida de peso duradera.
También puede ser aplicada a los pacientes tratados inicialmente con el método POSE.
Re-GESP es un procedimiento mínimamente invasivo, efectivo y duradero. Es una opción terapéutica real para el manejo de la obesidad y la reganancia de peso.
RETO / Endo-Sleeve
El Método de reparación endoscópica transoral RETO o endo-sleeve, consiste en la misma técnica de un Sleeve Gástrico Endoscópico mediante el sistema Apollo-Overstitch pero adaptado en los casos de reganancia de peso y dilatación posterior a la realización de un Sleeve laparoscópico.
La técnica consiste en aplicar suturas endoscópicas a lo largo de cuerpo gástrico dilatado para conseguir la reducción del diámetro del estómago.
Pacientes con bypass:
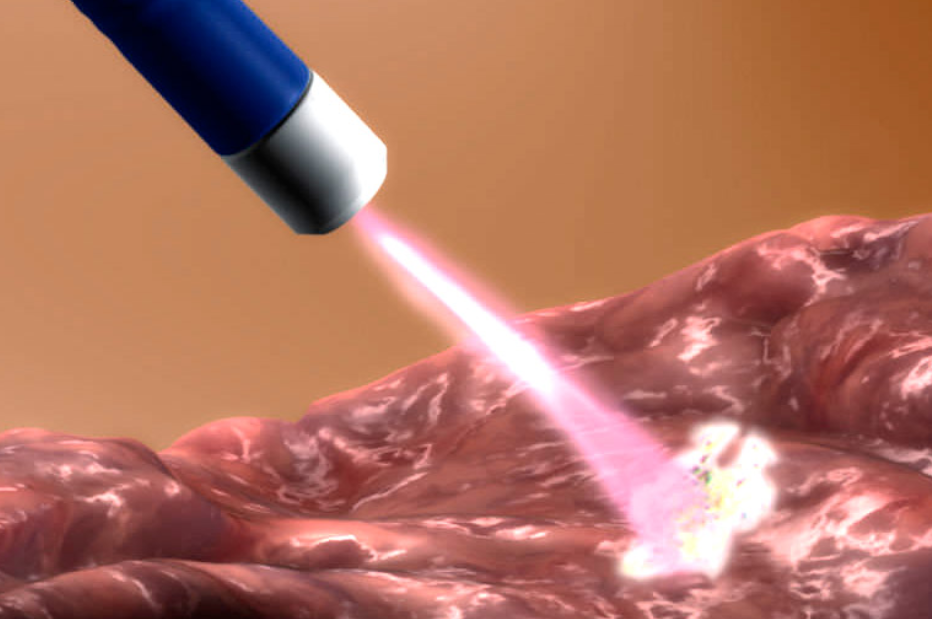
APC (Argón Plasma Coagulation)
La evidencia clínica muestra que algunos pacientes sometidos a bypass gástrico presentan usualmente dilatación de la boca anastomotica, es decir, la unión entre el remanente de estómago o pounch gástrico e intestino delgado, posteriormente esto sobrelleva a un constante aumento de peso.
Existen técnicas endoscópicas mínimamente invasivas después de la reganancia de peso en los pacientes de bypass gástrico, una de ellas es el APC o tratamiento con argón plasma.
La técnica consiste en utilizar argón plasma para promover la coagulación circunferencial de la anastomosis para disminuir su diámetro. En ocasiones es necesario complementar el procedimiento con la técnica Apollo Endosuture OverStitch agregando suturas endoscópicas, llamada también TORe (transoral outlet reduction endoscopy)
Ventajas:
Ambulatorio
Mínimamente invasivo
Rápida recuperación
TORe (Transoral outlet reduction endoscopy)
La reducción transoral del vaciamiento gástrico (TORe) o RETO como también se le conoce, es una técnica avanzada de endoscopia que utiliza el sistema Apollo Endosuture Overstich destinado para tratar los pacientes que con el tiempo recuperan parte del peso perdido posterior al bypass gástrico.
El TORe podría ser una alternativa válida y eficaz en estos pacientes.
La técnica consiste en aplicar suturas endoscópicas en la anastomosis para asegurar la aproximación de tejido y conseguir la reducción del diámetro de la anastomosis gastroyeyunal o unión del estómago y el intestino delgado.
Adicionalmente, pueden aplicarse otras suturas en el reservorio gástrico, en el caso en que esté dilatado, para favorecer una disminución de su volumen.
Ventajas:
Sin cirugía
Mínimamente invasivo
Rápida recuperación
ROSE (Restorative Obesity Surgery, Endoluminal).
La reducción endoscópica transoral o ROSE, también es otra técnica avanzada reparadora de la obesidad en pacientes que han regando peso.
Es efectiva para tratar de reducir la dilatación de la anastomosis o estoma gastro yeyunal hasta conseguir un diámetro aproximado de 10-15 mm, pero la aplicación de la técnica utiliza el método POSE.
Está indicado en aquellos pacientes que fueron intervenidos previamente mediante by-pass gástrico y han vuelto a ganar peso.
Ventajas de la técnica
– Sin ingreso hospitalario
– Sin incisiones